
Abstract
Background
In patients treated surgically for esophageal cancer, time-dependent data on nutritional status from the perioperative to postoperative period are questionable. We investigated time-dependent data on weight, body composition, and nutritional indices of patients with esophageal cancer from the preoperative period through the 12-month postoperative period.
Methods
Eighty patients with esophageal cancer were enrolled and subsequently underwent esophagectomy. Forty out of eighty patients were completed the 12-month follow-up survey period and analyzed. We assessed clinical, anthropometric measurement, laboratory data, and nutritional status data preoperatively and at 1, 3, 6, and 12 months postoperatively.
Results
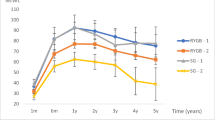
Patients with esophageal cancer had 7.2% weight loss in the preoperative period compared with the usual body weight (UBW) before morbidity and 9.3% weight loss from preoperative to 12-month postoperative period. Weight gain in the postoperative survey period was not significant. Conversely, there was a time lag in the time-dependent changes in the postoperative nutritional status; this was considered to coincide with internal organ protein, body protein, and body fat levels, in that order. Multivariate analysis identified a ≥ 10% preoperative weight loss compared with UBW as the only independent factor negatively contributing to ≥ 85% weight recovery at 12 months postoperatively (OR 6.54, 95% CI 1.14–37.60, p = 0.036).
Conclusions
For sufficient nutritional status recovery in patients treated with esophagectomy, minimizing weight loss preoperatively is important. Regardless of neoadjuvant therapy or age, preoperative nutritional treatment should be promptly administered for all patients.



Similar content being viewed by others


References
Kawasaki T, Sata T. Perioperative innate immunity. J UOEH. 2011;33:123–37.
Pedersen H, Hansen HS, Cederqvist C, et al. The prognostic significance of weight loss and its integration in stage-grouping of oesophageal cancer. Acta Chir Scand. 1982;148:363–6.
Onodera T, Goseki N, Kosaki G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. J Japan Surg Soc. 1984;85:1001–5.
O’Gorman P, McMillan DC, McArdle CS. Longitudinal study of weight, appetite, performance status, and inflammation in advanced gastrointestinal cancer. Nutr Cancer. 1999;35:127–9.
Guo SZ, Shen Q, Zhang HB. Expression and significance of immunosuppressive acidic protein (IAP) in human esophageal squamous cell carcinoma. Zhonghua Zhong Liu Za Zhi. 1994;16:125–7.
Ando N, Kato H, Igaki H, et al. A randomized trial comparing postoperative adjuvant chemotherapy with cisplatin and 5-fluorouracil versus preoperative chemotherapy for localized advanced squamous cell carcinoma of the thoracic esophagus (JCOG9907). Ann Surg Oncol. 2012;19:68–74.
Herskovic A, Martz K, Al-Sarraf M, et al. Combined chemotherapy and radiotherapy compared with radiotherapy alone in patients with cancer of the esophagus. N Engl J Med. 1992;326:1593–8.
Ettinger DS. Preventing chemotherapy-induced nausea and vomiting: an update and a review of emesis. Semin Oncol. 1995;22:6–18.
Martin L, Lagergren P. Long-term weight change after oesophageal cancer surgery. Br J Surg. 2009;96:1308–14.
Ouattara M, D’Journo XB, Loundou A, et al. Body mass index kinetics and risk factors of malnutrition one year after radical esophagectomy for cancer. Eur J Cardiothorac Surg. 2012;41:1088–93.
Carey S, Storey D, Biankin AV, et al. Long term nutritional status and quality of life following major upper gastrointestinal surgery—a cross-sectional study. Clin Nutr. 2011;30:774–9.
Shafer KJ, Siders WA, Johnson LK, et al. Validity of segmental multiple-frequency bioelectrical impedance analysis to estimate body composition of adults across a range of body mass indexes. Nutrition. 2009;25:25–32.
Sato M. Nutritional assessment of gastric cancer patients: estimation of risk of postoperative complication from preoperative nutritional states. J Japan Surg Soc. 1982;83:66–77.
Ignacio De Ulíbarri J, González-Madroño A, De Villar NGP, et al. CONUT: a tool for controlling nutritional status. First validation in a hospital population. Nutr Hosp. 2005;20:38–45.
Bauer J, Capra S, Ferguson M. Use of the scored Patient-Generated Subjective Global Assessment (PG-SGA) as a nutrition assessment tool in patients with cancer. Eur J Clin Nutr. 2002;56:779–85.
Koizumi M, Hosoya Y, Dezaki K, et al. Postoperative weight loss does not resolve after esophagectomy despite normal serum ghrelin levels. Ann Thorac Surg. 2011;91:1032–7.
Morgan DB, Paterson CR, Woods CG, et al. Search for osteomalacia in 1228 patients after gastrectomy and other operations on the stomach. Lancet. 1965;2:1085–8.
Tisdale MJ. Cachexia in cancer patients. Nat Rev Cancer. 2002;2:862–71.
Dewys WD, Begg C, Lavin PT, et al. Prognostic effect of weight loss prior to chemotherapy in cancer patients. Eastern Cooperative Oncology Group. Am J Med. 1980;69:491–7.
Moore FD. Metabolic care of the surgical patient. Philadelphia: WB Saunders Co; 1959. p. 421–2.
Chapman KM, Nelson RA. Loss of appetite: managing unwanted weight loss in the older patient. Geriatrics. 1994;49:54–9.
Okada G, Momoki C, Matsumoto Y, et al. The effects of preoperative weight loss on nutritional status and prognosis for esophageal cancer. J Gastroenterol Hepatol. 2016;3:026.
Ryan C, Bryant E, Eleazer P, et al. Unintentional weight loss in long-term care: predictor of mortality in the elderly. South Med J. 1995;88:721–4.
Schiffman SS. Taste and smell losses in normal aging and disease. JAMA. 1997;278:1357–62.
Ejaz A, Spolverato G, Kim Y, et al. Impact of body mass index on perioperative outcomes and survival after resection for gastric cancer. J Surg Res. 2015;195:74–82.
Martin L, Lagergren P. Risk factors for weight loss among patients surviving 5 years after esophageal cancer surgery. Ann Surg Oncol. 2015;22:610–6.
D’Journo XB, Ouattara M, Loundou A, et al. Prognostic impact of weight loss in 1-year survivors after transthoracic esophagectomy for cancer. Dis Esophagus. 2012;25:527–34.
Ottery FD. Supportive nutrition to prevent cachexia and improve quality of life. Semin Oncol. 1995;22:98–111.
Acknowledgements
The authors are grateful to J. Nadai, T. Hattori, S. Tsukada, and T. Fujii for constructive comments and warm encouragement. The authors would like to thank Enago (http://www.enago.jp) for the English language review.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Statement
All patients signed informed consent to participate in the study; the study received the approval of the Ethics Committee of Osaka City University Medical School (No. 1611). All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions.
Conflict of interest
Genya Okada, Yoshinari Matsumoto, Yoshihiro Nakamura, Fumikazu Hayashi, Kumiko Kato, Chika Momoki, Yoko Yasui, Daiki Habu, Eijiro Edagawa, Yasunori Matsuda, Satoru Kishida, Shigeru Lee, and Harushi Osugi declare that they have no conflicts of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Okada, G., Matsumoto, Y., Nakamura, Y. et al. Nutritional changes and factors contributing to postoperative weight recovery after esophagectomy. Esophagus 14, 343–350 (2017). https://doi.org/10.1007/s10388-017-0584-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10388-017-0584-6