Telomeric Repeat-Containing RNAs (TERRA) Decrease in Squamous Cell Carcinoma of the Head and Neck Is Associated with Worsened Clinical Outcome

 , , ,
, , ,
Abstract
:1. Introduction
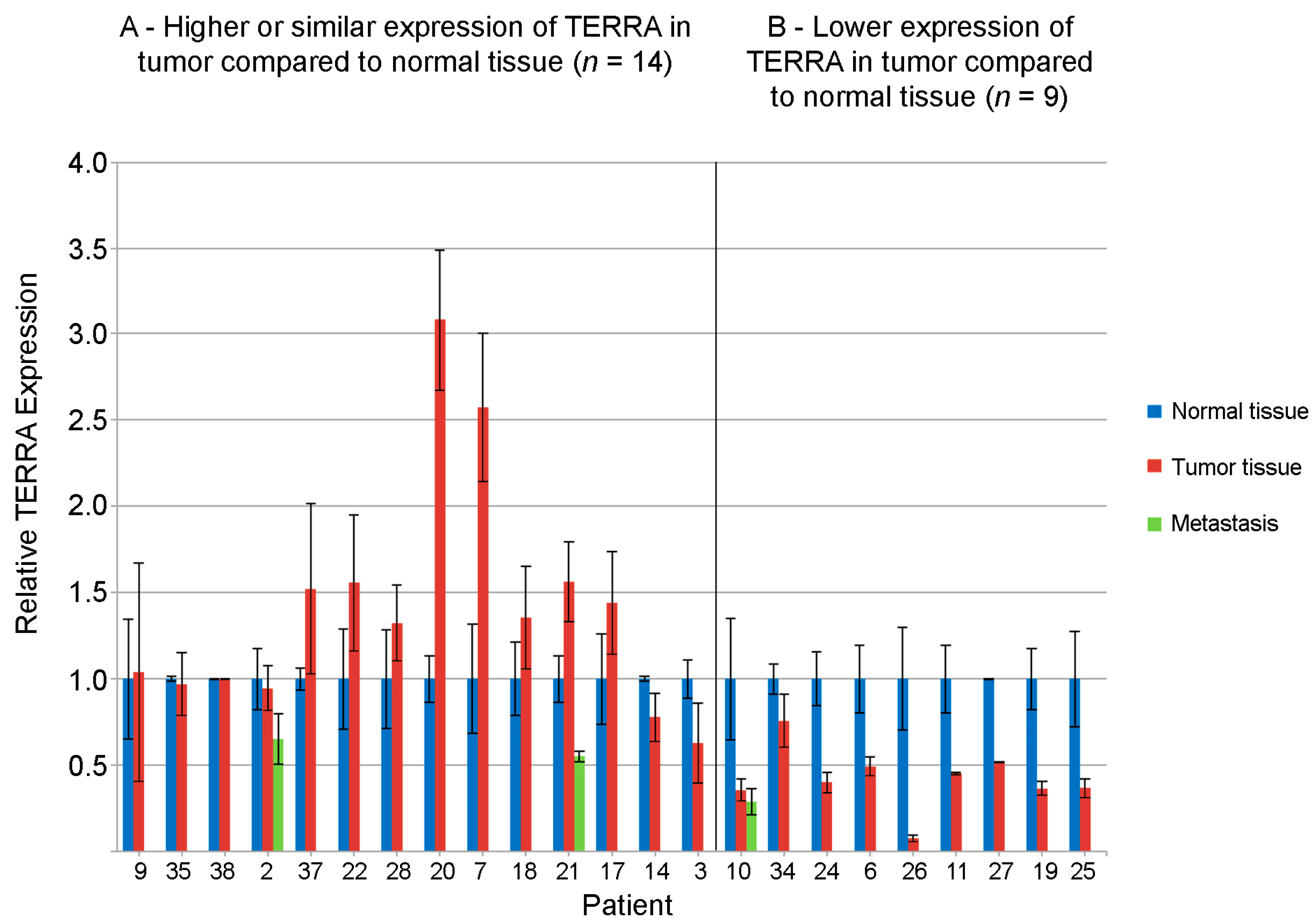
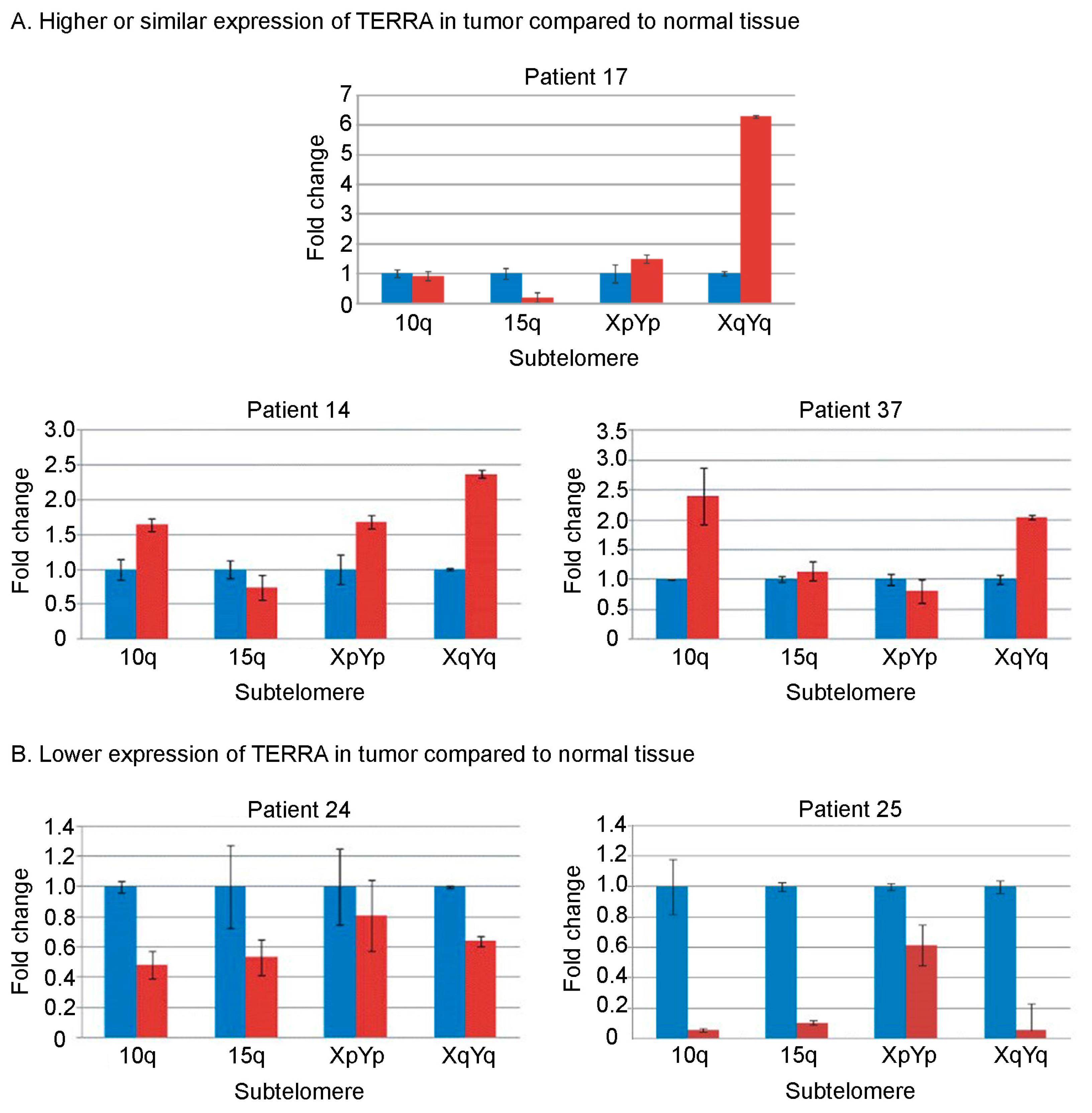
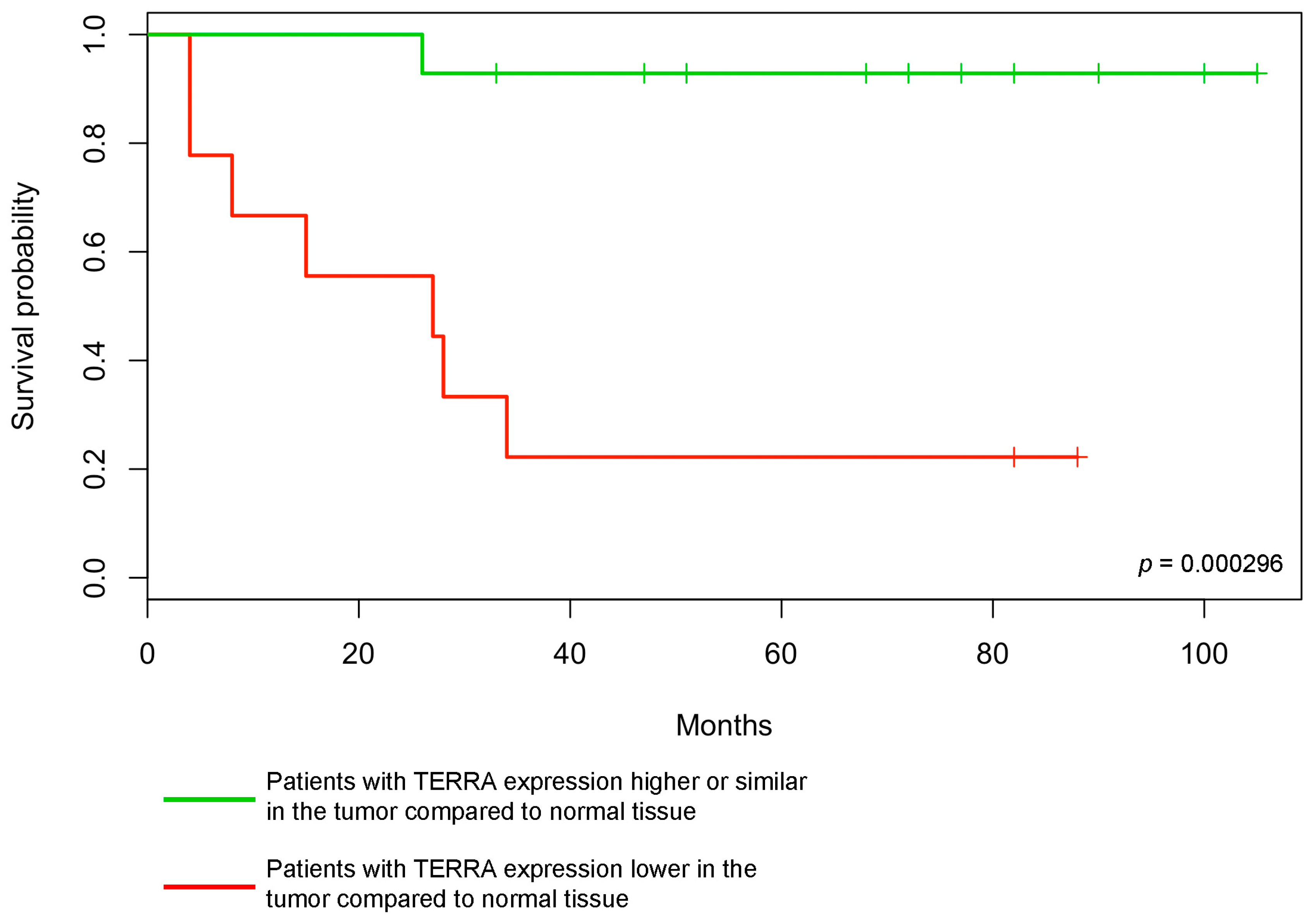
2. Results
3. Discussion
4. Materials and Methods
4.1. Patients Recruitment and Methods
4.2. RNA Extraction and Purification
4.3. Slot Blotting and Hybridization
4.4. Data Analysis
4.5. Reverse Transcription and qPCR
- U6-F, GGAACTCGAGTTTGCGTGTCATCCTTGCGC;
- U6-R, GGAATCTAGAACATATACTAAAATTGGAAC;
- 10q-F, CCGTTTGCTGCCCTGAATAA;
- 10q-R, TCTGACGCTGCACTTGAACC;
- 15q-F, CAGCGAGATTCTCCCAAGCTAAG;
- 15q-R, AACCCTAACCACATGAGCAACG;
- XpYp-F, GCAAAGAGTGAAAGAACGAAGCTT;
- XpYp-R, CCCTCTGAAAGTGGACCAATCA;
- XqYq-F, CCCCTTGCCTTGGGAGAA;
- XqYq-R, GAAAGCAAAAGCCCCTCTGA.
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| Ct | Threshold cycle |
| DFS | Disease-free survival |
| HCC | Hepatocellular carcinoma |
| HCV | Hepatitis C virus |
| HNC | Head and neck cancer |
| HNSCC | Head and neck squamous cell carcinoma |
| HPV | Human papilloma virus |
| pTNM | Pathological tumor node metastasis |
| qRT-PCR | Real-time quantitative polymerase chain reaction |
| RTFA | Radio-frequency thermal ablation |
| TERRA | Telomeric repeat-containing RNA |
References
- Palm, W.; de Lange, T. How shelterin protects mammalian telomeres. Annu. Rev. Genet. 2008, 42, 301–334. [Google Scholar] [CrossRef] [PubMed]
- Azzalin, C.M.; Reichenbach, P.; Khoriauli, L.; Giulotto, E.; Lingner, J. Telomeric repeat containing RNA and RNA surveillance factors at mammalian chromosome ends. Science 2007, 318, 798–801. [Google Scholar] [CrossRef] [PubMed]
- Schoeftner, S.; Blasco, M.A. Developmentally regulated transcription of mammalian telomeres by DNA-dependent RNA polymerase II. Nat. Cell Biol. 2008, 10, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Nergadze, S.G.; Farnung, B.O.; Wischnewski, H.; Khoriauli, L.; Vitelli, V.; Chawla, R.; Giulotto, E.; Azzalin, C.M. CpG-island promoters drive transcription of human telomeres. RNA 2009, 15, 2186–2194. [Google Scholar] [CrossRef] [PubMed]
- Deng, Z.; Norseen, J.; Wiedmer, A.; Riethman, H.; Lieberman, P.M. TERRA RNA binding to TRF2 facilitates heterochromatin formation and ORC recruitment at telomeres. Mol. Cell 2009, 35, 403–413. [Google Scholar] [CrossRef] [PubMed]
- Chawla, R.; Redon, S.; Raftopoulou, C.; Wischnewski, H.; Gagos, S.; Azzalin, C.M. Human UPF1 interacts with TPP1 and telomerase and sustains telomere leading-strand replication. EMBO J. 2011, 30, 4047–4058. [Google Scholar] [CrossRef] [PubMed]
- Arora, R.; Lee, Y.; Wischnewski, H.; Brun, C.M.; Schwarz, T.; Azzalin, C.M. RNaseH1 regulates TERRA-telomeric DNA hybrids and telomere maintenance in ALT tumour cells. Nat. Commun. 2014, 5, 5220. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.-Y.; Kao, Y.; Lin, J.-J. Telomeric transcripts stimulate telomere recombination to suppress senescence in cells lacking telomerase. Proc. Natl. Acad. Sci. USA 2014, 111, 3377–3382. [Google Scholar] [CrossRef] [PubMed]
- Azzalin, C.M.; Lingner, J. Telomere functions grounding on TERRA firma. Trends Cell Biol. 2015, 25, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Rippe, K.; Luke, B. TERRA and the state of the telomere. Nat. Struct. Mol. Biol. 2015, 22, 853–858. [Google Scholar] [CrossRef] [PubMed]
- Beishline, K.; Vladimirova, O.; Tutton, S.; Wang, Z.; Deng, Z.; Lieberman, P.M. CTCF driven TERRA transcription facilitates completion of telomere DNA replication. Nat. Commun. 2017, 8, 2114. [Google Scholar] [CrossRef] [PubMed]
- Chu, H.-P.; Cifuentes-Rojas, C.; Kesner, B.; Aeby, E.; Lee, H.-G.; Wei, C.; Oh, H.J.; Boukhali, M.; Haas, W.; Lee, J.T. TERRA RNA Antagonizes ATRX and Protects Telomeres. Cell 2017, 170, 86–101.e16. [Google Scholar] [CrossRef] [PubMed]
- Sampl, S.; Pramhas, S.; Stern, C.; Preusser, M.; Marosi, C.; Holzmann, K. Expression of telomeres in astrocytoma WHO grade 2 to 4: TERRA level correlates with telomere length, telomerase activity, and advanced clinical grade. Transl. Oncol. 2012, 5, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Deng, Z.; Wang, Z.; Xiang, C.; Molczan, A.; Baubet, V.; Conejo-Garcia, J.; Xu, X.; Lieberman, P.M.; Dahmane, N. Formation of telomeric repeat-containing RNA (TERRA) foci in highly proliferating mouse cerebellar neuronal progenitors and medulloblastoma. J. Cell Sci. 2012, 125, 4383–4394. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-J.; Chang, J.T.-C.; Liao, C.-T.; Wang, H.-M.; Yen, T.-C.; Chiu, C.-C.; Lu, Y.-C.; Li, H.-F.; Cheng, A.-J. Head and neck cancer in the betel quid chewing area: Recent advances in molecular carcinogenesis. Cancer Sci. 2008, 99, 1507–1514. [Google Scholar] [CrossRef] [PubMed]
- Friedlander, P.L. The use of genetic markers in the clinical care of patients with head and neck cancer. Arch. Otolaryngol. Head Neck Surg. 2003, 129, 363–366. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, J.P.; Suárez, C.; Ferlito, A.; Devaney, K.O.; Petruzzelli, G.J.; Rinaldo, A. Potential molecular prognostic markers for lymph node metastasis in head and neck squamous cell carcinoma. Acta Otolaryngol. 2003, 123, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Vikram, B.; Strong, E.W.; Shah, J.P.; Spiro, R. Failure at distant sites following multimodality treatment for advanced head and neck cancer. Head Neck Surg. 1984, 6, 730–733. [Google Scholar] [CrossRef] [PubMed]
- Gasco, M.; Crook, T. The p53 network in head and neck cancer. Oral Oncol. 2003, 39, 222–231. [Google Scholar] [CrossRef]
- Izzo, J.G.; Papadimitrakopoulou, V.A.; Liu, D.D.; den Hollander, P.L.C.; Babenko, I.M.; Keck, J.; El-Naggar, A.K.; Shin, D.M.; Lee, J.J.; Hong, W.K.; et al. Cyclin D1 genotype, response to biochemoprevention, and progression rate to upper aerodigestive tract cancer. J. Natl. Cancer Inst. 2003, 95, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Sturgis, E.M.; Wang, L.-E.; Chamberlain, R.M.; Amos, C.I.; Spitz, M.R.; El-Naggar, A.K.; Hong, W.K.; Wei, Q. Association of a p73 exon 2 G4C14-to-A4T14 polymorphism with risk of squamous cell carcinoma of the head and neck. Carcinogenesis 2004, 25, 1911–1916. [Google Scholar] [CrossRef] [PubMed]
- Gillison, M.L.; Koch, W.M.; Capone, R.B.; Spafford, M.; Westra, W.H.; Wu, L.; Zahurak, M.L.; Daniel, R.W.; Viglione, M.; Symer, D.E.; et al. Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. J. Natl. Cancer Inst. 2000, 92, 709–720. [Google Scholar] [CrossRef] [PubMed]
- Gleber-Netto, F.O.; Zhao, M.; Trivedi, S.; Wang, J.; Jasser, S.; McDowell, C.; Kadara, H.; Zhang, J.; Wang, J.; William, W.N.; et al. Distinct pattern of TP53 mutations in human immunodeficiency virus-related head and neck squamous cell carcinoma. Cancer 2018, 124, 84–94. [Google Scholar] [CrossRef] [PubMed]
- Lothaire, P.; de Azambuja, E.; Dequanter, D.; Lalami, Y.; Sotiriou, C.; Andry, G.; Castro, G.; Awada, A. Molecular markers of head and neck squamous cell carcinoma: Promising signs in need of prospective evaluation. Head Neck 2006, 28, 256–269. [Google Scholar] [CrossRef] [PubMed]
- Hui, L.; Wu, H.; Yang, N.; Guo, X.; Jang, X. Identification of prognostic microRNA candidates for head and neck squamous cell carcinoma. Oncol. Rep. 2016, 35, 3321–3330. [Google Scholar] [CrossRef] [PubMed]
- Wong, N.; Khwaja, S.S.; Baker, C.M.; Gay, H.A.; Thorstad, W.L.; Daly, M.D.; Lewis, J.S.; Wang, X. Prognostic microRNA signatures derived from The Cancer Genome Atlas for head and neck squamous cell carcinomas. Cancer Med. 2016, 5, 1619–1628. [Google Scholar] [CrossRef] [PubMed]
- Aida, J.; Izumo, T.; Shimomura, N.; Nakamura, K.-I.; Ishikawa, N.; Matsuura, M.; Poon, S.S.; Fujiwara, M.; Sawabe, M.; Arai, T.; et al. Telomere lengths in the oral epithelia with and without carcinoma. Eur. J. Cancer 2010, 46, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Boscolo-Rizzo, P.; Rampazzo, E.; Perissinotto, E.; Piano, M.A.; Giunco, S.; Baboci, L.; Spinato, G.; Spinato, R.; Tirelli, G.; Da Mosto, M.C.; et al. Telomere shortening in mucosa surrounding the tumor: Biosensor of field cancerization and prognostic marker of mucosal failure in head and neck squamous cell carcinoma. Oral Oncol. 2015, 51, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Boscolo-Rizzo, P.; Da Mosto, M.C.; Rampazzo, E.; Giunco, S.; Del Mistro, A.; Menegaldo, A.; Baboci, L.; Mantovani, M.; Tirelli, G.; de Rossi, A. Telomeres and telomerase in head and neck squamous cell carcinoma: From pathogenesis to clinical implications. Cancer Metastasis Rev. 2016, 35, 457–474. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.Y.; Lin, S.C.; Chang, C.S.; Wong, Y.K.; Hu, Y.C.; Chang, K.W. Telomerase activity and in situ telomerase RNA expression in oral carcinogenesis. J. Oral Pathol. Med. 1999, 28, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Curran, A.J.; Gullane, P.J.; Irish, J.; Macmillan, C.; Freeman, J.; Kamel-Reid, S. Telomerase activity is upregulated in laryngeal squamous cell carcinoma. Laryngoscope 2000, 110, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Fabricius, E.-M.; Gurr, U.; Wildner, G.-P. Telomerase activity levels in the surgical margin and tumour distant tissue of the squamous cell carcinoma of the head-and-neck. Anal. Cell. Pathol. 2002, 24, 25–39. [Google Scholar] [CrossRef] [PubMed]
- Meeker, A.K.; Hicks, J.L.; Iacobuzio-Donahue, C.A.; Montgomery, E.A.; Westra, W.H.; Chan, T.Y.; Ronnett, B.M.; De Marzo, A.M. Telomere length abnormalities occur early in the initiation of epithelial carcinogenesis. Clin. Cancer Res. 2004, 10, 3317–3326. [Google Scholar] [CrossRef] [PubMed]
- Smirnova, A.; Gamba, R.; Khoriauli, L.; Vitelli, V.; Nergadze, S.G.; Giulotto, E. TERRA expression levels do not correlate with telomere length and radiation sensitivity in human cancer cell lines. Front. Oncol. 2013, 3, 115. [Google Scholar] [CrossRef] [PubMed]
- Vitelli, V.; Falvo, P.; Khoriauli, L.; Smirnova, A.; Gamba, R.; Santagostino, M.; Nergadze, S.G.; Giulotto, E. More on the lack of correlation between TERRA expression and telomere length. Front. Oncol. 2013, 3, 245. [Google Scholar] [CrossRef] [PubMed]
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tân, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N. Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Licitra, L.; Rossini, C.; Bossi, P.; Locati, L.D. Advances in the changing patterns of aetiology of head and neck cancers. Curr. Opin. Otolaryngol. Head Neck Surg. 2006, 14, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Morbini, P.; Alberizzi, P.; Tinelli, C.; Paglino, C.; Bertino, G.; Comoli, P.; Pedrazzoli, P.; Benazzo, M. Identification of transcriptionally active HPV infection in formalin-fixed, paraffin-embedded biopsies of oropharyngeal carcinoma. Hum. Pathol. 2015, 46, 681–689. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2016. [Google Scholar]
- Schneider, C.A.; Rasband, W.S.; Eliceiri, K.W. NIH Image to ImageJ: 25 years of image analysis. Nat. Methods 2012, 9, 671–675. [Google Scholar] [CrossRef] [PubMed]
- ImageJ Documentation. Dot Blot Analysis. Available online: http://imagej.nih.gov/ij/docs/examples/dot-blot/index.html (accessed on 30 April 2009).
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2−ΔΔCt Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| No. | Sex/Age | Tumor Site | Staging (pTNM) | Grading | HPV Status | Date of Sampling | Status at 15 December 2017 | DFS (Months) |
| A | ||||||||
| 9 | F/71 | Oropharynx | T4a, N0, M0 | G2 | Negative | 15 April 2011 | Dead of disease on 24 June 2013 | 26 |
| 35 | M/67 | Oropharynx | T3, N0, M0 | G2 | Negative | 1 March 2012 | Alive. On 15 December 2014, a second primary tumor (SCC of the tongue staged pT2, N2, M0, graded G2) was resected | 33+ |
| 38 | M/64 | Tongue | T2, N0, M0 | G2/G3 | ND | 16 December 2013 | Alive, disease-free | 48+ |
| 2 | M/70 | Hypopharynx | T4a, N2b, M0 | G2 | ND | 10 September 2013 | Alive, disease-free | 51+ |
| 37 | M/66 | Oropharynx | T4a, N0, M0 | G1/G2 | Negative | 26 March 2012 | Alive, disease-free | 68+ |
| 22 | M/68 | Tongue | T3, N0, M0 | G2 | ND | 12 April 2010 | Lost at follow-up on 9 May 2016, when was alive and disease-free | 72+ |
| 28 | F/79 | Larynx | T3, N0, M0 | G2/G3 | ND | 15 July 2011 | Alive, disease-free | 77+ |
| 20 | M/59 | Larynx | T4a, N0, M0 | G2 | ND | 8 February 2011 | Alive, disease-free | 82+ |
| 7 | M/55 | Larynx | T4a, N0, M0 | G2 | ND | 24 January 2011 | Alive, disease-free | 82+ |
| 18 | M/79 | Hypopharynx | T2, N2, M0 | G2/G3 | ND | 17 January 2011 | Alive, disease-free | 82+ |
| 21 | M/72 | Tongue | T3, N1, M0 | G2/G3 | ND | 1 June 2010 | Alive, disease-free | 90+ |
| 17 | M/52 | Oropharynx | T2, N0, M0 | G2 | Negative | 24 May 2010 | Alive, disease-free | 90+ |
| 14 | M/59 | Larynx | T4a, N0, M0 | G2 | ND | 20 July 2009 | Alive, disease-free | 100+ |
| 3 | M/52 | Pharynx | T4a, N0, M0 | G3/G3 | ND | 26 February 2009 | Alive, disease-free | 105+ |
| B | ||||||||
| No. | Sex/Age | Tumor Site | Staging (pTNM) | Grading | HPV Status | Date of Sampling | Status at 15 December 2017 | DFS (Months) |
| 10 | M/65 | Cervical esophagus | T2, N0, M1 (liver) | G2 | ND | 24 October 2013 | Dead of disease on 21 March 2014 | 4 |
| 34 | F/77 | Hypopharynx | T3, N0, M0 | G2 | ND | 26 November 2010 | Dead of disease on 6April 2011 | 4 |
| 24 | F/71 | Oropharynx | T4a, N1, M0 | G2 | Negative | 21 February 2011 | Dead of disease on 19 November 2011 | 8 |
| 6 | M/59 | Hypopharynx 1 | T4a, N0, M0 | G2 | ND | 20 October 2011 | Dead of disease on 10 February 2013 | 15 |
| 26 | M/70 | Oropharynx 1 | T2, N0, M0 | G2 | Negative | 7 July 2011 | Dead of disease on 22 October 2013 | 27 |
| 11 | M/58 | Tongue | T3, N1, M0 | G2 | ND | 28 September 2009 | Dead of disease on 10 February 2012 | 28 |
| 27 | F/63 | Tongue | T3, N0, M0 | G2 | ND | 11 July 2011 | Dead of disease on 18 May 2014 | 34 |
| 19 | M/70 | Larynx | T4a, N2, M0 | G2 | ND | 31 January 2011 | Alive, disease-free (for head and neck tumor). On 6 March 2017 a second primary tumor (hepatocellular carcinoma, HCC) on a chronic HCV (hepatitis C virus) infection was diagnosed. The HCC was treated by means of RTFA and has not recurred to date. | 82+ |
| 25 | F/62 | Larynx 1 | T2, N2, M0 | G2 | ND | 19 July 2011 | Alive, disease-free | 88+ |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vitelli, V.; Falvo, P.; G. Nergadze, S.; Santagostino, M.; Khoriauli, L.; Pellanda, P.; Bertino, G.; Occhini, A.; Benazzo, M.; Morbini, P.; et al. Telomeric Repeat-Containing RNAs (TERRA) Decrease in Squamous Cell Carcinoma of the Head and Neck Is Associated with Worsened Clinical Outcome. Int. J. Mol. Sci. 2018, 19, 274. https://doi.org/10.3390/ijms19010274
Vitelli V, Falvo P, G. Nergadze S, Santagostino M, Khoriauli L, Pellanda P, Bertino G, Occhini A, Benazzo M, Morbini P, et al. Telomeric Repeat-Containing RNAs (TERRA) Decrease in Squamous Cell Carcinoma of the Head and Neck Is Associated with Worsened Clinical Outcome. International Journal of Molecular Sciences. 2018; 19(1):274. https://doi.org/10.3390/ijms19010274
Chicago/Turabian StyleVitelli, Valerio, Paolo Falvo, Solomon G. Nergadze, Marco Santagostino, Lela Khoriauli, Paola Pellanda, Giulia Bertino, Antonio Occhini, Marco Benazzo, Patrizia Morbini, and et al. 2018. "Telomeric Repeat-Containing RNAs (TERRA) Decrease in Squamous Cell Carcinoma of the Head and Neck Is Associated with Worsened Clinical Outcome" International Journal of Molecular Sciences 19, no. 1: 274. https://doi.org/10.3390/ijms19010274